![]() COVID-19 ALERT: Find COVID-19 Testing Sites. COVID-19 Vaccine Info. New Visitor Policy. Make a Donation.
COVID-19 ALERT: Find COVID-19 Testing Sites. COVID-19 Vaccine Info. New Visitor Policy. Make a Donation.
Abstract
- Issue: Health systems often lack resources to support intensive efforts that emphasize prevention. A contributing factor is the continued dependence on fee-for-service reimbursement. All-payer global hospital budgeting is a promising innovation that departs from fee-for-service reimbursement by assuring a hospital receives a prospectively set amount of revenue over the course of the year. This assurance creates an incentive to reorganize care delivery and invest in services to address preventable health conditions.
- Goals: Assess the feasibility and likely outcomes of implementing global all-payer budgets in hospital systems in the United States, particularly in large safety-net hospital systems.
- Methods: Analysis of concepts based on the experiences of global hospital budgeting programs implemented in Maryland and planned for Pennsylvania.
- Key Findings and Conclusions: To be successful, all-payer global hospital budgeting requires a vision for transformation, an operational strategy, and an environment conducive to success. Key considerations for adopting this approach include whether alternative payment methods can accomplish the same goals, whether a sufficient reference population can be defined to guide year-over-year budget adjustments, and whether a strong governance structure can be established and sustained.
Background
Many communities in the United States experience high rates of premature illness and death.1 In 2015, the nation’s life expectancy dropped for the first time since 1993.2
Expanding access to primary care, behavioral health services, and other social services can improve health outcomes and moderate rising costs. However, finding sustainable sources of funding for clinical transformation has been challenging. One major reason is that the safety-net health care systems still depend on fee-for-service reimbursement for hospital services. When health systems can stay afloat only by keeping inpatient beds filled, major investments in prevention can sink the ship.
All-Payer Global Hospital Budgeting
An emerging payment innovation is all-payer global hospital budgeting. This approach involves an annual expectation for revenue for all inpatient and hospital outpatient care in advance, creating a powerful incentive to reorganize care for prevention and to invest in community services.
The use of all-payer global hospital budgeting as a public policy tool in the United States began in Maryland.3 In 2010, Maryland’s independent rate-setting agency launched a pilot program for 10 rural hospitals, in which each was guaranteed a set amount of revenue for the coming year, regardless of the number of inpatient admissions, emergency department visits, and other volume measures.4 Chief executives of the pilot hospitals discovered that the new all-payer global budget model freed them from the urgent need to keep their beds filled to maintain adequate revenue.5 These hospitals launched new multidisciplinary clinics to care for individuals with chronic disease, enhanced transitions of care, and supported new programs for behavioral health.6
In 2014, Maryland and the Centers for Medicare and Medicaid Services (CMS) announced a payment model that expanded all-payer global budgets to all 46 acute care hospitals in the state.7 The initial evaluation by CMS found that the state was already making progress on aggregate hospital expenditures, clinical quality, and readmissions:
By several measures, this evaluation found the first 18 months of Maryland All-Payer Model implementation was a success. Acute-care hospitals in the state transitioned to global budgets more quickly than projected, and most hospitals successfully managed their revenues to remain within the 0.5 percent corridor around their global budget.
The evaluation also reported, “These findings are particularly notable because they reflect early experience with the All-Payer Model, when hospitals were just beginning to adjust to the new system. Discussions with hospital leaders during site visits indicated that in most cases hospitals were in the early stages of developing strategies to respond to the incentives of the All-Payer Model. In particular, strategies that require changes outside the hospital’s direct control — such as aligning hospital and physician incentives and reducing patient demand for hospital services by improving population health and altering care-seeking patterns — were in the nascent stages.”8
After 30 months, Maryland has seen a 48 percent reduction in potentially preventable complications, and has seen the readmission rate fall from 7.9 percent to 3.4 percent over the national average.9 In addition, after nearly three years of operation, the results include $429 million in hospital savings in Medicare compared to the national rate of growth, which has translated to a $319 million total cost-of-care savings relative to national Medicare trends.
Even as Maryland’s model is still in its early stages, interest in all-payer global hospital budgeting is growing among rural hospitals. Notably, in January 2017, Pennsylvania and CMS announced a payment model that will bring an all-payer global hospital budgeting model to 30 rural hospitals within three years.10 The idea of a global budget is particularly attractive for small, geographically isolated facilities that are struggling to maintain adequate volume to survive under fee-for-service reimbursement.11 Under a global budget, a rural hospital can plan for a set amount of revenue and invest in “outside the walls” initiatives to reduce preventable hospital utilization.
Large safety-net health systems in urban areas differ in many respects from small rural hospitals. Their challenge may be too many patients, not too few, and their reach may be far beyond inpatient services into a network of community clinics. In addition, the proximity of urban safety-net hospitals to competing health systems means that a portion of their patients may have readily accessible alternatives for obtaining care. However, there is an important commonality: Both rural hospitals and large safety-net hospitals frequently adopt strong social missions for their communities that include efforts to address major sources of preventable illness.
This report assesses the potential of all-payer global hospital budgeting to meet the challenges large safety-net health systems and their communities face. We describe the steps necessary for developing all-payer global budgets and identify key considerations for all-payer global budgeting in the context of alternative strategies for value-based payment. To illustrate how global budgeting might be applied in an urban area, we also highlight the experiences of NYC Health + Hospitals, New York City’s network of public safety-net hospitals and affiliated community clinics.
Implementing All-Payer Global Budgets in Large Safety-Net Hospitals
There are three primary steps to implementing all-payer global budgets in large safety-net hospitals: a vision for transformation, an operational strategy, and an environment conducive to success.
Step 1: A Vision for Transformation
To overcome the political and policy challenges involved in establishing all-payer global hospital budgeting, a health system must promote a strong vision for transformation that can earn support from three audiences: the local community, key state and federal policymakers, and the staff at the health system itself.
A successful vision begins with combining an assessment of community health challenges with an understanding of the limitations of the current financial model in addressing them. A local analysis might find, for example, that in a specific population, infant mortality rates are high, preventable asthma admissions are frequent, and opioid-related overdoses are rising. It might then note that the health system does not have adequate financial resources to invest in expanding health services, such as primary care, evidence-based home visiting, behavioral health treatment, and care coordination for complex patients. It should explain the unfortunate dynamic that success in reducing admissions, under the current payment model, would have significant adverse financial consequences.
The vision should then define a set of promising initiatives that would be possible under an all-payer hospital budget that guarantees revenue independent of inpatient volume. These might include:
- Additional primary care and community-based behavioral health services;
- hanges in hospital service lines, depending on community needs;
- Care coordination for high-need patients;
- Effective use of health information technology to identify high-need, high-cost patients and areas in need of additional support12; and
- Coordination with local public health agencies and other community resources around primary prevention and investments in addressing social determinants of health.
Such efforts are a key focus of transformation activities at many safety-net hospitals, including NYC Health + Hospitals.
The vision should also include ways to align with local physicians, including opportunities for doctors to earn incentives under both the Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model tracks of the Medicare and CHIP [Children’s Health Insurance Program] Reauthorization Act. The complex reporting requirement in the Merit-Based Incentive Payment pathway provides opportunities for health systems to align interests with independent physicians who are seeking assistance in meeting the requirements. The Alternative Payment Model track could enhance existing efforts and investments to align with primary care physicians in new payment models for patient-centered medical homes to address community needs. In addition, new bundled payment programs provide opportunities for specialists to join high-value health care networks. Because community primary care and specialty physicians play a vital role in managing chronic illness, this alignment is essential for success over the long term.
Transformation Activities at NYC Health + Hospitals
To improve health outcomes and lower costs, with the support of funds made available through the state’s Medicaid waiver, NYC Health + Hospitals is pursuing:
- Primary care improvement. The health system is standardizing patient panels; seeking medical home certification for dozens of practices; expanding phone access; and improving quality oversight using metrics for cardiovascular disease, diabetes, and depression.
- Community health collaboration. For example, in collaboration with community partners, the health system has promoted pre-exposure prophylaxis for HIV and engaged community health workers to support patients with asthma.
- Identification and care for high-need patients. The system has developed a risk-scoring algorithm that can identify high-need patients for care coordination and other services.
- Behavioral health integration. Pilots for improved care of depression, anxiety, and substance use disorders are under way.
Sustainability and expansion of these efforts will require a mechanism to capture and reinvest savings from the prevention of inpatient hospitalizations.
Sources: Correspondence from OneCity Health. Also see The City of New York, One New York: Health Care for Our Neighborhoods. Transforming Health + Hospitals (City of New York, 2016).
The vision should address why it is important for all payers to participate: It permits the clinical system to fully transform to emphasize prevention and disease management, rather than maintain two or more delivery systems within the same hospital attuned to different incentives. Another important reason is that full participation would create benefits for everyone in a community, regardless of their source of payment for health care.
Finally, the vision for transformation should include metrics for success. One such metric is the financial viability of the safety-net health system itself. Others might include:
- Improvements in community health outcomes, such as overdose;
- Reductions in preventable inpatient admissions;
- Reductions in hospital-acquired conditions;
- Reductions in readmissions; and
- Increased use of effective outpatient services, such as evidence-based addiction treatment.
A vision for transformation should begin as a high-level concept that shows communities, political leaders, public agencies, and private payers what a different set of financial incentives for the acute care hospital can help accomplish. It can then evolve over time into a detailed implementation plan.
Step 2: An Operational Strategy to Manage Global Budgets
In addition to a vision of health and transformation for a hospital and its community, all-payer hospital global budgeting requires an operational strategy for the system itself. Such a strategy should define 1) how budgets will be established and adjusted over time; 2) how payers will participate; and 3) how an effective structure for governance and administration will be established.
How budgets will be established and adjusted over time
An all-payer global hospital budget is not guaranteed to stay at a set level indefinitely; if it were, a health system could succeed financially simply by directing its patients elsewhere. To avoid this perverse incentive, a global budgeting system needs a set of rules to adjust the global budget year over year, based in part on patient preference represented by market shifts, as well as demographic and other trends.
Initial Global Budgets
A hospital’s first global budget is most easily set through a review of historical patterns of expenditures. This approach, which is straightforward to implement and acceptable to hospital leadership, was rapidly implemented in Maryland across dozens of hospitals.
Adjustments to Global Budgets Each Year
Establishing a fair process for adjustments to global budgets each year is a key step for preserving key incentives while maintaining stability for the participating hospitals. These adjustments should be based in part on 1) the ongoing experience of a specific reference population that can be closely monitored and 2) the utilization of services by others who are not part of this reference population.
Reference population. The concept of a reference population is critical for all-payer hospital global budgeting in the United States. This is the population most closely tracked for year-over-year budget adjustments. At the most basic level, if this reference population is growing in number, the hospital receives a larger budget to provide care. A global budgeting system can also make year-over-year adjustments based on trends in the demographics and health status of the reference population.
It is worth noting that the concept of a reference population distinguishes U.S. all-payer global hospital budgeting from global hospital budgeting in Canada and Europe, which generally set hospital budgets based on the characteristics of the provider, such as the number of beds or types of services offered.13
Adjustments to global budgets based on the reference population are designed to address the concern over perverse incentives to direct patients elsewhere. If the reference population moves to other institutions for essential care, then the hospital will experience a reduction in its global budget over time.14 On the other hand, if the reference population is becoming healthier, with fewer preventable admissions, the hospital will enjoy a stable budget even in the setting of declining utilization.
Who is in the reference population? Maryland’s approach, the only one implemented to date in the United States, uses the population living in the hospital’s service area. Maryland has developed methods to account for overlapping service areas in urban and suburban regions. Pennsylvania’s rural hospital program will also use geography-based reference populations.
An alternative approach for the reference population could be to include individuals assigned by specific payers or attributed on the basis of primary care affiliation. For example, the population could include all enrollees in an accountable care organization (ACO) affiliated with the hospital, or all patients of a set of primary care physicians. The greater the number of attributed patients through either mechanism, the greater the corresponding part of the global budget. The fewer participants, the smaller the budget. Should preferences among patients shift toward or away from the hospital, the budget would increase or decrease, respectively.
Such alternative approaches to geography-based reference populations may be difficult to implement. Models that attribute individuals to a specific provider are the main methods used to build populations for ACOs, but establishing clear linkages between a single physician and a hospital may be more difficult and may change over time.
Other populations of patients. For those patients who are seen by the hospital but are not part of the reference population, revenues can be included in the budget each year and then adjusted for future years depending on utilization. For example, the Maryland system adjusts some global budgets based on fluctuations in non-state-resident utilization (Exhibit 1).
Exhibit 1
Addressing Changes Over Time
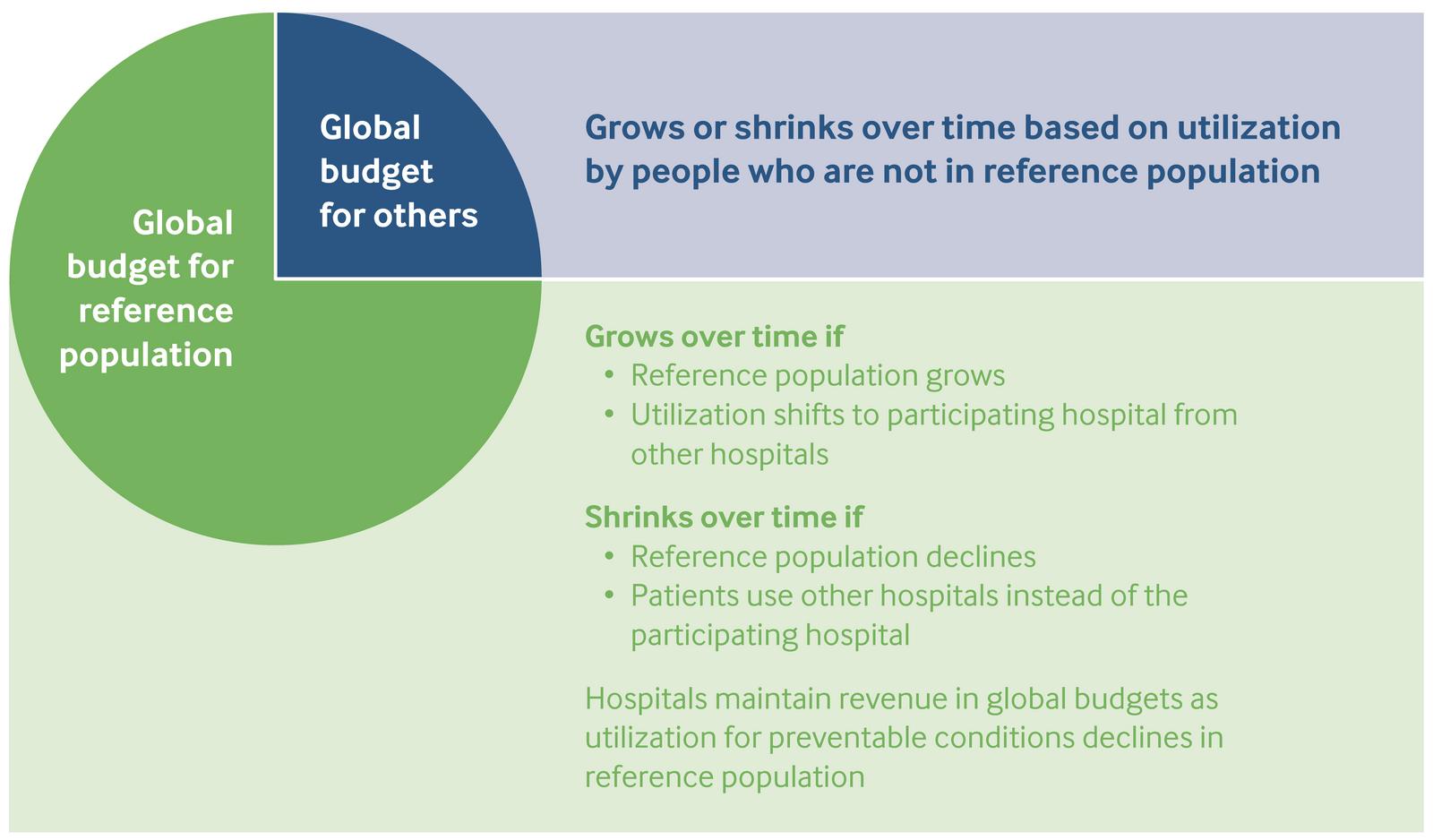
Source: J. M. Sharfstein, S. Gerovich, E. Moriarty et al., An Emerging Approach to Payment Reform: All-Payer Global Budgets for Large Safety-Net Hospital Systems, The Commonwealth Fund, August 2017.
In theory, these two approaches to defining a reference population could be combined and include both a local and an attributed population. Finding a relatively large reference population is critically important to the success of hospital global budgeting.
Adjustments to global hospital budgets over time can also take into account metrics that reflect the quality of care, population health outcomes, and patient experience. These can be implemented by setting benchmarks in advance or by rewarding hospitals that produce continuous improvement over time.
How payers will participate
A global budget without payer participation is like a party without guests. Fortunately, there are several ways to divide the responsibility for hospital budgets among participating payers. In Maryland, payers continue to make claim-based payments based on the rates determined by the rate-setting agency; the rate-setting agency works behind the scenes with hospitals to adjust rates to accomplish global budgeting, effectively turning the rate-setting mechanism into a cost allocation method.
Global budgeting is also possible without rate-setting, with payers contributing to each hospital’s revenues each year based on their historic utilization of the hospital’s services. This contribution must also be adjusted each year.
Medicare
Given the frequency with which older adults require hospital care, Medicare’s participation is essential to the establishment of a global budgeting program. This participation is made possible by a waiver to hospital payment rules issued by the Center for Medicare and Medicaid Innovation at the request of the state. The waiver sets the terms under which Medicare pays the assigned share of global budgets to particular hospitals. Because Medicare fee-for-service spending is relatively predictable over time, it is not difficult to transition to global budget payments.15
The Importance of the Reference Population
The reference population serves as the core target for health improvement activities. If preventable admissions decline in this population, the hospital maintains the revenue.
It is therefore critical that the reference population be as large as possible. If just 5 percent of the population of a hospital is in a reference population, then there will be few opportunities to invest in prevention and keep the benefit. If 95 percent of the population of a hospital is in a reference population, then clinical transformation will bring many rewards.
For this reason, adoption of an all-payer hospital global budgeting strategy may be accompanied by a strategy to increase the reference population. For example, if a reference population is based on primary care attribution, a health system may choose to invest in more primary care physicians.
Medicaid
Given the importance of Medicaid reimbursement for safety-net hospitals, Medicaid participation in a global budgeting program is also essential. States have considerable flexibility under both the Medicaid statute and the 1115 waiver process to change the terms of hospital payment.16 Like Medicare, Medicaid can chart trends and convert expected payments into global payments for a population.17
Indirect public payments should be included under global budgets. These payments, which may represent a large proportion of health system revenues, include Disproportionate Share Hospital (DSH) payments and Upper Payment Limit (UPL) payments.
- DSH payments are intended to compensate hospitals that care for large low-income populations. These are set at the federal level and distributed among qualifying hospitals by the state, based on a broad range of factors that include past levels of inpatient volume. Medicaid DSH payments are due to shrink considerably under the terms of the Affordable Care Act, although these declines have so far been postponed.
- UPL payments are state payments to hospitals permitted in Medicaid so long as the total reimbursement for classes of providers does not exceed what Medicare would reimburse. These payments often support hospitals with links to entities (such as county governments) that contribute directly to the Medicaid program.
Traditional DSH and UPL payments have been linked to inpatient utilization, consistent with the fee-for-service paradigm of traditional hospital payment. Recently, however, there has been growing interest in incorporating such funds in value-based payment arrangements.18 Under an 1115 waiver, a state can consolidate the DSH and UPL programs in order to contribute to hospital global budgets. California’s recent 1115 waiver renewal includes a “global budget” program that is limited to the uninsured; the program sets a maximum global budget for each hospital that is provided in proportion to the services delivered to this population.19
Including DSH and UPL payments in all-payer hospital global budgets strengthens the alignment of incentives for clinical transformation.
Global Budgeting Without Rate-Setting
Pennsylvania’s proposed approach to global budgeting involves assigning an appropriate proportion of a negotiated global budget to each payer. For example, if a hospital’s negotiated budget is $100 million and the share of hospital expenditure attributable to Insurer A’s patients is consistently 35 percent, then Insurer A might be directed to pay the hospital $35 million over the course of the year. This payment could be arranged on a monthly or quarterly basis.
At the end of the year, if Insurer A’s actual percentage of volume is different from 35 percent, there could be an adjustment in the current or following period.
How an effective structure for governance and administration will be established
An essential component of an all-payer global hospital budgeting model is a strong governance structure with an effective approach to implementation. Maryland’s hospital payment model is managed by the Health Services Cost Review Commission, an independent agency created by Maryland statute whose members are appointed by the governor. No more than three members of the seven-member panel may have provider affiliations, and, by tradition, at least one comes from the physician community.20 Pennsylvania is planning to create a Rural Health Redesign Center as a public-private partnership to perform a similar function.
It is essential that the administering agency have credibility with key public and private partners. If seen as a purely political creation, the agency will not be trusted to be fair. If it tilts too far toward payers or toward hospitals, one or the other may lose confidence in the system’s ability to succeed. In addition, an expert staff is essential to generating data-driven analyses to understand the system and respond quickly to problems as they arise.
As noted above, effective administration of an all-payer global hospital budgeting program involves the setting and adjusting of global budgets with a transparent and fair set of methodologies. It also includes assigning contributions to payers, monitoring market shifts, assessing quality, and measuring outcomes. There is also a range of other operational considerations. An administering agency can exempt certain expensive, unusual services, such as burn units and transplants, from all-payer global budgets. It can handle capital investments differently from other costs. It can penalize inappropriate behavior, such as inappropriate facility transfers. Budgets can also be adapted to account for other factors, such as the costs of medical technology and pharmaceuticals beyond the hospital’s control. The administering agency must be able to adjust budgets when extraordinary situations, such as a severe influenza season, demand additional spending. It can be anticipated that the operations of the governance structure will cost at least several million dollars a year.
Step 3: An Environment Conducive to Success
No health system is an island; success under all-payer global budgeting depends on a variety of market and policy factors. Three critical factors are the local hospital environment, the engagement of the state government, and the availability of an information technology infrastructure, technical assistance, and startup funding.
Local hospital environment
An urban environment may include large safety-net health systems as well as private systems that may be less likely to serve the same number of low-income patients. A critical question for a large safety-net hospital considering a global budget is whether surrounding hospitals will also shift to this method of payment. A hospital is far more likely to meet its goals under a global budget if neighboring hospitals serving the same or a similar population are also paid under global budgets.
A regional ecosystem of global budgeting has several benefits. First, it eliminates the danger that the other hospitals would seek out additional volume to grow their revenue, which may mean reductions in global budgets due to what appear to be market shifts. Second, it creates an incentive for collaboration in addressing the needs of high-need patients, because reductions in preventable admissions would benefit all facilities. Third, it allows payers to look across larger populations to see trends in utilization and cost, providing more confidence about the progress of the model. And finally, it creates additional synergy with local public health agencies interested in defined geographic populations. An example of a possible regional global budgeting system is shown in the box at the right.
Engagement of the state government
State officials play a central role in establishing any system of all-payer hospital global budgeting, including for large safety-net systems. This role is in part because of formal authority. Not only, as noted above, does Medicare participation depend on a request from the state, but participation of the state Medicaid program is also essential for success. Beyond formal authority, strong state leadership, including that of the governor, is needed to encourage transformation, align payers, and set expectations for reform.
Engaging state officials starts with the vision for transformation. State leaders may see special value in the alignment of global budgeting with public health goals for specific geographic areas or populations, such as reducing overdose, addressing chronic illness, and helping older adults age in place. They may also see value in using all-payer global hospital budgets to align the long-term incentives of health systems and hospitals with other innovations in payment that aim to reduce preventable illness and associated costs, including patient-centered medical homes, accountable care organizations, and system investments through the Delivery System Reform Incentive Program (DSRIP).21 These state officials may have longstanding, constructive relationships with the leadership of safety-net health systems that can serve as a foundation for discussion.
Of note, Medicaid participation in a global hospital budgeting program differs fundamentally from a “block grant” from the federal government to the state. Under a block grant, the federal government imposes a financial cap that supersedes all other factors. This limitation can erode financial support for the Medicaid program over time and may make it impossible to meet core patient care obligations.
By contrast, an all-payer global hospital budgeting program has the primary purpose of improving health. The model is developed with multiple safeguards and a governance structure to ensure that innovative financial incentives are used to achieve improvements in care for patients and health for local communities. If these incentives fail to do so, then public agencies, private payers, and local communities can revert to the previous basis of payment.
Could All-Payer Global Hospital Budgeting Work in the Bronx?
The Bronx is a county with 1.46 million people, a poverty rate of 31.5 percent, and the second-highest rate of preventable admissions in New York. While an individual hospital could move to a global budget, there would be a risk that the surrounding hospitals could increase their own volumes correspondingly and undermine their success.
An alternative would be for all Bronx hospitals to be paid under global budgets, allowing payers to monitor the success of the initiative across all Bronx residents. At the county level, over 90 percent of people admitted to Bronx hospitals in 2014 were Bronx residents. Moreover, about 75 percent of hospital admissions for Bronx residents in 2014 occurred in Bronx hospitals.
Bringing all the hospitals together under global budgeting could allow for the design of a transformed health system with alignment for the health of the population and with the engagement of community leaders and public health agencies.
Source: SPARCS Hospital Data, New York State Department of Health.
Availability of an information technology infrastructure, technical assistance, and startup funding
The administering agency requires access to high-quality data on hospital utilization and, to the extent possible, tools for identifying opportunities for health systems to improve outcomes and lower costs. For example, Maryland’s health information exchange helps identify patients with complex health needs, sends real-time alerts to clinicians, and provides rapid reporting to hospitals on readmissions.
In addition, health systems often need technical and financial support to transition into alignment with new incentives under all-payer global budgets. As a committee of the National Academy of Medicine recently noted, “Even when there is financial alignment, organizations with fewer resources may not be able to respond … without upfront resources.”22 Pennsylvania is receiving $25 million from CMS to provide technical assistance and other support through the new Rural Health Redesign Center. Other sources of funding include private philanthropy, foundations, and the global budgets themselves, which can be set to provide additional room for population health investments. Maryland provided hospitals with additional resources in the first two years of the state’s program.
Alternatives Innovative Payment Arrangements and Other Considerations for Safety-Net Hospitals
Safety-net health systems are much more than essential providers of acute care. As community institutions aiming to maximize the health and well-being of those they serve, these organizations recognize the urgency of investments in prevention. Yet fee-for-service reimbursement and outdated approaches to indirect payments in the Medicaid program can box these health systems into dependency on inpatient volume for revenue.
In theory, an all-payer global hospital budgeting program can provide safety-net health systems the flexibility to achieve their financial and population health goals. In practice, there are several important questions that relate to the viability of this model for particular areas.
An important consideration is whether there are alternative and more readily available payment mechanisms capable of achieving the same transformational results. One reason the Medicaid managed care program started several decades ago was to encourage greater attention to preventive care. However, a major limitation of managed care has been the separation of the payer from the provider, so that health systems are unable to capture savings that can sustain transformation. There are efforts in some states, including New York, to require managed care plans to pass incentives to clinical systems capable of managing risk. This may create new opportunities for large urban safety-net systems.
Another recent development is the rise of accountable care organizations in the Medicaid program. Massachusetts, Rhode Island, and Vermont all have 1115 waivers under Medicaid to support risk sharing by health systems acting as accountable care organizations.
The use of this tool can be part of an “a la carte” approach to value-based payment, along with structuring payment for the uninsured so that it is not based on inpatient volume. Patching together such a system without a single global budget does not require the degree of public and private coordination needed for an all-payer hospital global budgeting program. A key consideration, however, is whether the patchwork covers an adequate share of patient volume seen by inpatient facilities. If it fails to do so, health systems can be stuck with the proverbial “one foot in each canoe,” unable to transform to leave fee-for-service medicine behind. Furthermore, a patchwork approach may create undesirable challenges for risk management, if patients move back and forth between value-based and fee-for-service reimbursement.
A more logistical consideration is whether health systems can identify a viable reference population upon which to base a global budgeting strategy. Those that can team up with other public and private hospitals as part of a global budgeting program in their region may be best placed to succeed.
For an individual hospital considering a global budget, a key question is whether there is a defined service area that supplies a large number of patients. If this is not the case, and the hospital draws diffusely from a diverse area, such as across an entire city, it may be difficult to identify a reference population based on geography. In such a case, the feasibility of a global budget may depend on the ability to identify an attributed or assigned population and develop sophisticated approaches to tracking market shifts.
A third consideration is whether there is a path to a credible administrator for an all-payer global hospital budgeting system. Long-standing disputes between hospitals or between hospitals and insurers may complicate the development and implementation of an all-payer global hospital budgeting model. Well-trusted private or quasi-public agencies are best suited for taking on such a role. The leadership of such organizations will need to bring in professional staff to provide oversight to the system in a credible fashion.
Conclusion
All-payer hospital global budgeting is an emerging payment reform that can permit large safety-net health systems to make major investments in community health. This approach can complement and sustain other value-based reforms at the state level. Developing a successful financial and delivery model requires a vision for transformation, an operational strategy, and an environment conducive to success.
Safety-net health systems interested in exploring this potential funding innovation may choose to consider the following steps:
- Describe the challenge. Assess the level of avoidable hospitalizations and corresponding savings that might be possible under a global budget.
- Draft a vision for transformation. Develop specific proposals to reduce avoidable hospitalization that could be made sustainable under a global budget.
- Propose an operational strategy. Study the local health care environment to identify potential reference populations to use as the basis for hospital global budgeting.
- Discuss with policymakers. Start talking about all-payer global hospital budgeting with local, state, and federal elected representatives and health officials.
- Imagine a governance structure. Consider what characteristics may make the most sense locally and be most credible.
- Consider alternatives. Evaluate all options to promote greater alignment among financial incentives, community health, and hospital sustainability.
For their part, local and state officials may choose to learn more about global hospital budgeting to address long-standing challenges facing safety-net health systems and their communities.
Notes
1 National Academy of Sciences, Engineering, and Medicine, Systems Practices for the Care of Socially At-Risk Populations (National Academies Press, 2016).
2 L. Bernstein, “U.S. Life Expectancy Declines for the First Time Since 1993,” Washington Post, Dec. 8, 2016.
3 Clinical systems such as Kaiser Permanente and the Veterans Health Administration have set hospital budgets for many years. Both systems have been able to make significant investments in prevention and see the results reflected in lower expenditures with equal or better quality.
4 In Maryland, the only state that sets hospital rates, the commission created this “global budget” by allowing these 10 hospitals to adjust their all-payer rates up or down, depending on whether the actual rate of admissions came in under or over what had been expected.
5 B. Ronan, “Total Patient Revenue,” The Ronan Report, April 27, 2011.
6 J. M. Sharfstein, D. Kinzer, and J. M. Colmers, “An Update on Maryland’s All-Payer Approach to Reforming the Delivery of Health Care,” JAMA Internal Medicine, July 2015 175(7):1083–84.
7 Key financial components of this model included 1) a limit on the growth of per capita hospital expenditures for all payers to 3.58 percent per capita, the long-term trend of growth of the state’s economy; and 2) a lower rate of growth in per capita hospital expenditures for Maryland residents in the Medicare program compared with the national average, so that the state will save Medicare at least $330 million over five years. R. Rajkumar, A. Patel, K. Murphy et al., “Maryland’s All-Payer Approach to Delivery-System Reform,” New England Journal of Medicine, Feb. 6, 2014 370(6):493–95.
8 S. Haber, H. Beil, W. Adamache et al., Evaluation of the Maryland All-Payer Model: First Annual Report (RTI International, Oct. 2016).
9 N. Sabatini, J. Antos, H. Haft et al., “Maryland’s All-Payer Model — Achievements, Challenges, and Next Steps,” Health Affairs Blog, Jan. 31, 2017.
10 Centers for Medicare and Medicaid Services, Pennsylvania’s Rural Health Model (CMS, n.d.).
11 J. M. Sharfstein, “Global Budgets for Rural Hospitals,” Milbank Quarterly, June 2016 94(2):255–59.
12 Maryland benefits from the Chesapeake Regional Information System for Our Patients, a health information exchange that permits patient lookup and real-time notification for clinicians across the state.
13 W. Quentin, D. Scheller-Kreinsen, M. Blümel et al., “Hospital Payment Based on Diagnosis-Related Groups Differs in Europe and Holds Lessons for the United States,” Health Affairs, April 2013 32(4):713–23. Hospitals in these countries are generally prohibited from spending funds from their global budgets on new community-based services designed to reduce utilization of inpatient care.
14 Both Maryland and Pennsylvania are expecting to achieve Medicare savings in hospital costs for their reference populations.
15 Medicare Advantage plans are more complicated. There may be a number of competing plans with rapid changes in market share and hospital payment. The administering authority can ask these plans to contribute to global budgets in proportion to their use of hospital services during the calendar year.
16 In Maryland, the state’s Medicaid program participates in all-payer hospital global budgeting through the state’s Medicaid plan without special provisions in a 1115 waiver.
17 Also like Medicare, managed care organizations can be expected to contribute to global budgets in proportion to their use of hospital services.
18 C. Mann, D. Bachrach, A. Lam et al., Integrating Medicaid Supplemental Payments into Value-Based Purchasing (The Commonwealth Fund, Nov. 2016).
19 California Association of Public Hospitals and Health Systems and California Health Care Safety Net Institute, Issue Brief: The Global Payment Program — Improving Care for the Uninsured in California’s Public Health Care Systems (CAPH/SNI, July 2016).
20 Maryland Health Services Cost Review Commission, HSCRC Overview (HSCRC, n.d.).
21 The DSRIP program is a type of 1115 Medicaid waiver that provides substantial funding for community health investments in exchange for specific commitments to a series of process and outcome metrics. See: A. Gates, R. Rudowitz, and J. Guyer, An Overview of Delivery System Reform Incentive Payment (DSRIP) Waivers (Henry J. Kaiser Family Foundation, Oct. 2014).
22 National Academies of Science, Engineering, and Medicine, Systems Practices for the Care of Socially At-Risk Populations (National Academies Press, 2016), p. 57.